|
HIV prevention research: progress and challenges in the new millennium
Steve Bende* and Anthony S. Fauci
National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, Maryland 20892, United States
*To whom correspondence should be addressed. Present address: Generic Pharmaceutical Association, 1620 I St., NW, Suite 800, Washington, District of Columbia 20006, United States. Phone: (202) 833-9070; FAX (202) 833-9612; Email: Steve.Bende@GPHAonline.org.
Introduction
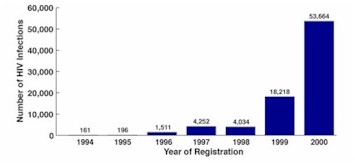
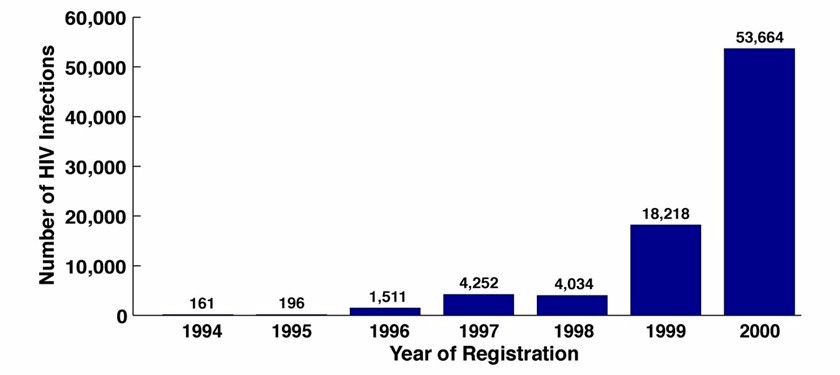
Despite recent advances in treatment and prevention, human immunodeficiency virus (HIV) disease and the acquired immunodeficiency syndrome (AIDS) continue to exact an enormous toll throughout the world (1, 2). More than 58 million people worldwide have been infected with HIV since the beginning of the pandemic, and 22 million of these individuals have died. Globally, about one in every 100 adults aged 15 to 49 is HIV-infected. An estimated 5.3 million people were infected with HIV in the year 2000 alone, mostly in developing countries (Figure 1). Sub-Saharan Africa bears the greatest burden of the epidemic; more than 70 percent of all HIV-infected individuals live in that region. In 16 African countries, the prevalence of HIV infections among adults aged 15 to 49 exceeds 10 percent. HIV infection in other regions is also cause for great concern. The Caribbean region has rates of HIV infection that are the highest in the world outside of Africa. In Asia, the number of HIV cases has risen sharply in recent years, notably in China and India. HIV infections also have escalated sharply in certain countries of the former Soviet Union (Figure 2).
 |
| [View larger version of this image] |
| Figure 1. Newly registered HIV infections in Russia, 1994 to 2000. Cases reported through January 17, 2001 (Source: Russian Federal AIDS Center, Moscow). |
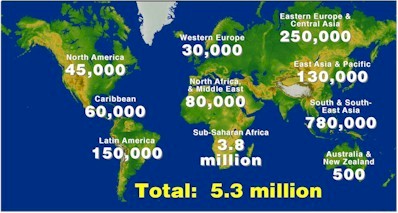 |
| Figure 2. Estimated number of new HIV infections by region in 2000 (Source: reference 1). |
In addition to its human toll, AIDS has had a profound negative impact on social and economic development, diminishing the economic viability and, potentially, the political stability of countries with high rates of infection (1, 2).
In the United States, an estimated 800,000 to 900,000 people are living with HIV disease; another 440,000 HIV-infected people have died (3, 4). The number of new infections in the United States has reached an unacceptable plateau of approximately 40,000 per year, with minority populations disproportionately affected, especially poor people in inner-city areas (3, 4).
Potent combinations of anti-HIV drugs (highly active antiretroviral therapy or "HAART") have reduced the number of AIDS deaths and new AIDS cases in many western countries, but these drugs are unavailable in most poor countries due to cost and lack of public health infrastructure (1, 2). Even in settings where antiretroviral drugs are available and (relatively) affordable, their utility is limited by toxicities, complicated dosing regimens, and the development of drug resistance (5). Paradoxically, in the United States the availability of these medications may be a contributing factor in the recent resurgence of HIV risk behaviors among gay men, as individuals may mistakenly believe that HIV disease is now an easily managed condition (6).
These realities underlie the urgency of developing effective and affordable tools of HIV prevention. In this discussion, we briefly highlight some of the progress and challenges in HIV prevention research, with a focus on several programs of the National Institute of Allergy and Infectious Diseases (NIAID), a component of the U.S. National Institutes of Health.
Key Areas of Prevention Research
Historically, vaccines have provided safe, cost-effective, and efficient means of preventing illness, disability, and death from infectious diseases. The development of a safe and effective vaccine for HIV infection is a central goal of AIDS research and a necessary tool to bring the HIV pandemic under control. Considerable efforts have been mounted in the search for an HIV vaccine, and numerous vaccine candidates are in various stages of pre-clinical and clinical development (see below). In addition, a number of non-vaccine approaches to HIV prevention have been pursued by researchers and public health officials (Table 1), including education and behavior modification; treatment of substance abuse; treatment of other sexually transmitted diseases (STDs); and the development of topically-applied microbicides (7).
|
| Table 1. Approaches to HIV Prevention |
|
| 1. | Interruption of transmission from mother to child |
| 2. | Interruption of transmission from adult to adult via antiretroviral therapy |
| 3. | Education and behavior modification |
| 4. | Drug abuse treatment (e.g., methadone) |
| 5. | Condoms and clean syringes |
| 6. | Topical microbicides |
| 7. | Treatment of other sexually transmitted diseases |
| 8. | Vaccination |
|
Prevention of maternal-fetal transmission
Some of the most notable successes in HIV prevention research have resulted from trials of antiretroviral treatment to prevent transmission of HIV from mother to infant. In a pivotal study known as Pediatric AIDS Clinical Trials Group (PACTG) 076, administration of zidovudine (AZT) to the mother before, during and after labor, and to the baby for 6 weeks after delivery, led to a 67% reduction in HIV transmission (8). Subsequently, simpler regimens have been assessed; for example, a study conducted in Thailand found that a brief course of AZT, given only before and during labor, still reduced the rate of perinatal transmission by 50 percent (9). More recently, investigators in Uganda found that giving a single dose of nevirapine to the HIV-infected mother at inception of labor and a single dose to the neonate within 72 hours of birth resulted in similar reductions in transmission rates, at a significantly reduced cost (Figure 3) (10). In a follow-up to this study, investigators of the HIV Prevention Trials Network (HPTN) are exploring the use of nevirapine therapy in infants from birth to 6 months of age to prevent transmission of HIV from mothers during breastfeeding.
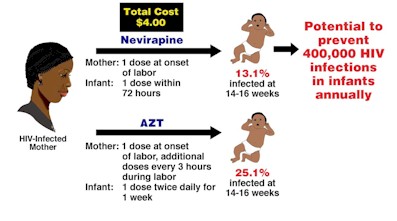 |
| Figure 3. Nevirapine therapy of mother and neonate to prevent mother-to-infant transmission: the HIVNET 012 trial in Uganda (See reference 10). |
Topical Microbicides
Physical barrier methods, notably latex condoms, are effective measures against the sexual transmission of HIV and other pathogens, and have been invaluable in slowing the progression of the epidemic. Indeed, aggressive programs of education and condom promotion have been credited with slowing the trajectory of the HIV epidemic in western countries, as well as in Uganda, Thailand and other countries with strong programs of AIDS prevention (1, 2, 3). However, the use of condoms (both male and female) ultimately requires the consent and cooperation of sexual partners, and at-risk individuals frequently cannot negotiate their use. Therefore, researchers are developing alternate methods of blocking HIV and other sexually transmitted pathogens. Such microbicides may be in the form of microbicidal gels, foams, creams or films for vaginal or rectal application, or for penile application using treated "wipes" (11). Although many candidate microbicides have potent activity against transmitted pathogens in vitro and in animals, their efficacy has yet to be proven in clinical trials. A number of practical issues challenge microbicide researchers, including affordability, stability, formulation flexibility to allow development of contraceptive and non-contraceptive forms, minimization of effects on vaginal ecology, and acceptability to users with regard to tactile and other sensory qualities. Despite these obstacles, a useful topical microbicide can be developed, and NIAID has a strong commitment to microbicide research and development.
Treatment of Other Sexually Transmitted Diseases
Individuals with a sexually transmitted disease (STD) are at increased risk of acquiring HIV, and those with HIV are more likely to transmit the virus when they have concomitant STDs (12). Early detection and treatment of other STDs may decrease HIV transmission in certain settings. In this regard, improved STD treatment reduced HIV incidence by about 40% in a rural population in Tanzania in which the epidemic was relatively newly established (13). In a subsequent study, researchers of the Rakai Study Group in Uganda found no effect of a community based STD intervention on the incidence of HIV-1 infection in a setting where the epidemic was more entrenched or "mature" (14). These and others studies suggest that treatment of STDs may reduce the risk of HIV infection for an individual, and for a population if the intervention is initiated before or soon after the establishment of the epidemic. However, in a mature epidemic, treatment of STDs may have an impact only after a prolonged period (15).
While the Rakai study was seen by some as disappointing, it has provided additional insights into the transmission of HIV as well as possible approaches to prevention. For example, circumcised men enrolled in the study had a significantly reduced risk of acquiring HIV infection (16). Perhaps most importantly, the Rakai investigators found viral load to be the best predictor of heterosexual HIV transmission (17). There were no instances of HIV transmission among the 51 subjects with serum HIV-1 RNA levels less than 1,500 copies per milliliter of blood and a significant dose-response relationship existed between increased transmission and increasing viral load. This finding has encouraged therapeutics and vaccine researchers alike. Although the ultimate goal of HIV therapy is improved health through the restoration of an individual’s immune status, the lowering of viral load might slow the epidemic by decreasing the likelihood of transmission. With regard to vaccine development, these and other data suggest that sterilizing immunity might not be absolutely necessary for a vaccine to be useful; a vaccine that reduced viral load might also have a significant impact not only for the individual but also in terms of reducing transmission (Figure 4).
 |
[View larger version of this image] |
| Figure 4. Potential effect of vaccination on the course of HIV disease. An HIV vaccine that reduces viral "set point" in vaccinated individuals subsequently infected with HIV may be useful. |
Vaccines
The development of a safe and effective HIV vaccine clearly is paramount to halting the AIDS epidemic. Perhaps the greatest obstacle to vaccine development is an insufficient understanding of the correlates of immune protection, which are better understood for other viral diseases. Other challenges include the high rate of HIV mutation within populations and individuals, suboptimal animal models, the poor immunogenicity and high variability of the HIV envelope protein, persistence of latent infection, and the potential requirement for both systemic and mucosal protection.
Despite these obstacles, there are many reasons for optimism in the search for an HIV vaccine. Notably, individuals who become infected with HIV typically do not develop AIDS for years even in the absence of anti-retroviral therapy, suggesting that the human immune system is capable of partially controlling HIV infection. Potential correlates of immunity have been illuminated by recent studies and provide insights into vaccine design. In this regard, data suggest that the initial control of viremia during the acute phase of infection is mediated by HIV-specific cytotoxic T lymphocytes (CTLs) (18, 19). Other cellular immune responses, including the secretion of CC-chemokines by CD8+ T cells may confer a protective effect (20). In some HIV-infected individuals who have failed to progress to AIDS, researchers have identified potent antigen-specific CD4+ T cell proliferative responses (21). In addition, passive transfer of virus-specific monoclonal antibodies to non-human primates has protected these animals from infection or lessened the severity of their disease, providing evidence for the potentially protective effects of neutralizing antibodies (22-24).
Another reason for optimism is that a number of vaccine candidates have protected non-human primates from infection and/or progression of disease (25). The most robust protection has been associated with live-attenuated simian immunodeficiency virus vaccines containing deletions in one or more regions of the viral genome. Unfortunately, when the protected animals were tracked for an extended period after immunization, or when these attenuated viruses were inoculated into neonatal monkeys, AIDS eventually developed (26). Nonetheless, protection in the SIV model provides investigators with an opportunity to delineate the correlates of protection in these animals, and hopefully information on the design of an effective HIV vaccine.
The NIAID HIV Vaccine Trials Network (HVTN), formerly the AIDS Vaccine Evaluation Group, has provided a wealth of clinical data that contribute to the concept that an AIDS vaccine can be developed. Most encouraging have been observations that candidate vaccines tested to date appear to be safe, and a number have induced potent immune responses. In addition, CTLs from vaccinated volunteers have shown potent activity ex vivo against multiple clades of HIV (27). Among many projects, the HVTN is exploring the use of "prime-boost" regimens to induce both cellular and humoral arms of the immune system. Virus vectors engineered from canarypox virus containing one or more HIV genes have proved to be safe and can stimulate CTL responses in vaccinated individuals. Subsequent immunization with recombinant envelope gp120 has resulted in significant levels of HIV-specific antibodies in these same vaccinees (28).
Currently, NIAID is considering plans to perform an efficacy trial using the prime-boost approach. In addition, a robust commitment to HIV vaccine development has greatly expanded the "pipeline" of vaccine candidates (Table 2). Indeed, we hope to soon have the luxury of choosing among several strong vaccine candidates to move into efficacy trials.
|
| Table 2. Examples of Candidate HIV/AIDS Vaccines In Development (Source: reference 29). |
|
| Vaccine | Example |
| DNA | DNA plasmids |
| Live viruses | Adeno-associated virus |
| Herpesvirus |
| Vaccinia |
| Canarypox |
| Modified vaccinia Ankara |
| Yellow fever |
| Replicons | Alphaviruses (VEE, Sindbis, Semiliki) |
| Poliovirus |
| Bacteria | Salmonella |
| Listeria |
| Shigella |
| BCG |
| Whole-killed | HIV inactivated by multiple methods |
| Live-attenuated | HIV with gene deletions |
| Recombinant subunit | Envelope (oligomeric, polyvalent, etc.) |
| Regulatory proteins (tat, etc.) |
| Epitope-based | Peptides |
| Polyepitope |
| Psuedovirions/virus-like particles | p55 gag |
| Adjuvant/immunomodulator | |
| Cytokines (protein or DNA) | IL-2 |
| IL-12 |
| IL-15 |
| GM-CSF |
| Costimulatory molecules | B7 |
| CD40L |
| Delivery vehicles | Synthetic microparticles |
| Mucosa-specific (cholera toxin, etc.) |
|
Conclusion
As the AIDS epidemic continues to devastate communities in the developed and developing world, the search for affordable, practical methods to prevent this deadly infection remains a critical public health priority. Great strides have been made, especially with regard to blocking perinatal transmission and with behavioral interventions. Increased support of preclinical AIDS vaccine research has filled the AIDS vaccine pipeline with many new approaches. The NIAID has established a dedicated clinical trials network, the HVTN, to perform the trials necessary to evaluate these approaches. New tools of HIV prevention and a sustained commitment to HIV prevention research are critical to our efforts to contain the AIDS epidemic.
References and notes
|

{kind=link}
{kind=link}